Posterior Thigh (Hamstrings) Excision
It is a procedure that involves removing a tumor (usually malignant or benign aggressive) of the posterior thigh (hamstring muscles) while preserving the surrounding bone and soft tissues.

It is a procedure that involves removing a tumor (usually malignant or benign aggressive) of the posterior thigh (hamstring muscles) while preserving the surrounding bone and soft tissues.
The posterior compartment of the thigh (hamstrings) is the least common site of the three compartments of the thigh (anterior, posterior, medial) for soft tissue tumors to arise. Approximately 15% to 20% of soft tissue sarcomas around the thigh arise in the posterior hamstring compartment. The major muscles of the posterior thigh (hamstring muscles) include the biceps femoris, semimembranosus, and semitendinosus muscles. Although resection of the muscular elements of this compartment does not considerably affect overall function of the lower extremity, the proximity of the major nerves, arteries, and veins of the lower extremity to this area requires special attention in the preoperative evaluation process and during tumor removal. Some of the most common types of soft tissue tumors that arise in this site include lipomas and low-grade liposarcomas. High-grade soft tissue sarcomas may adhere to some of the vascular structures (veins and arteries) and require careful dissection and preservation of the femoral (femur) vessels. About 90% of soft tissue sarcomas arising in the anterior thigh (quadriceps muscles) can be resected and treated adequately by a limb-sparing surgery. In some instances the extremity cannot be saved and an amputation is performed.
Contraindications for saving the limb may include neurovascular invasion, infection, pathological fracture, invasion of the pelvic floor, extensive disease, contamination from a poorly performed biopsy, recurrent disease.
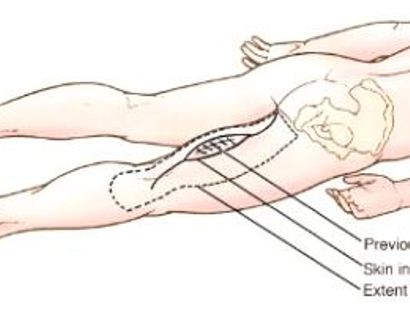
A long incision is made in the back of the leg, and if a previous biopsy was done the area will be marked as seen in the image.
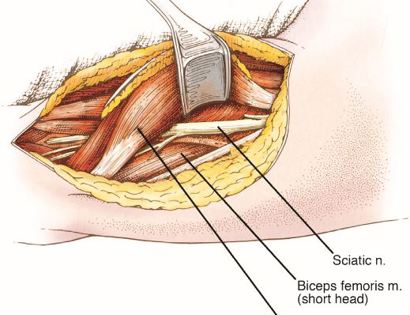
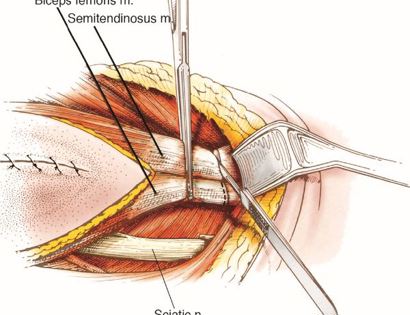
The skin flaps are created and pulled away as well as the long head femoris muscle to expose important contents of the back of the leg including the sciatic nerve.
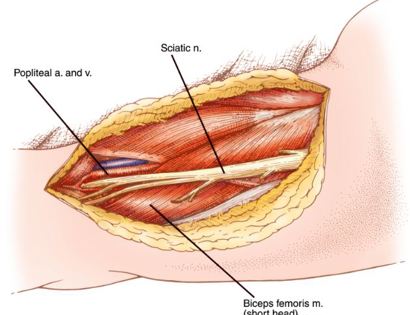
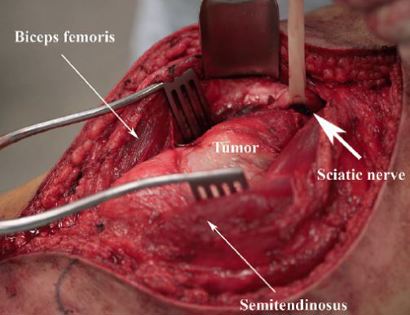
Separating all major arteries, veins, and nerves from the tumor. In rare cases a nerve (s) may need to be removed if it is involved by the sarcoma. For this type of procedure, it is vital that the sciatic nerve and femoral artery and vein are properly identified and mobilized away from the tumor. Once the blood vessels and nerves are separated, they can be retracted (moved away from the tumor) and protected throughout the procedure.
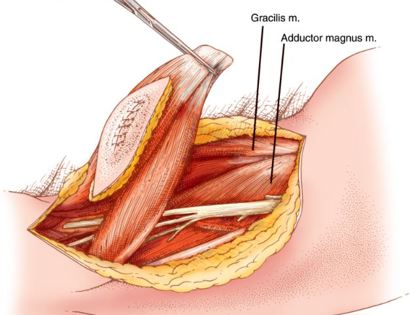
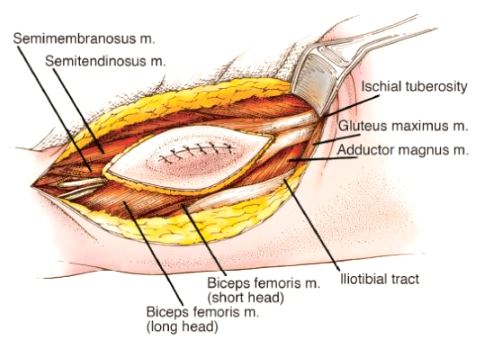
Developing surgical planes (margins that are tumor free) and separating muscles such as the gracilis and adductor magnus that can be preserved and leaving those such as the biceps femoris and semitendinosus in continuity with the tumor that should be removed. This is based on preoperative MRI and intraoperative findings as well as the type of tumor.
The hamstrings are removed with the tumor starting at the point at which the muscle inserts into the bone.
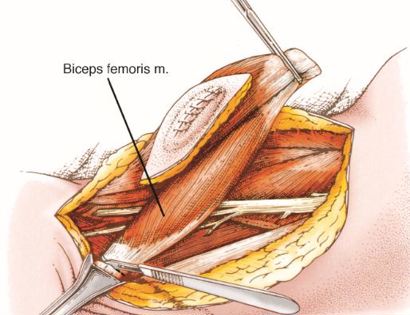
The biceps femoris is removed with the tumor in tact. The tumor is located within the skin ellipse found on the surface of the semitendinosus.
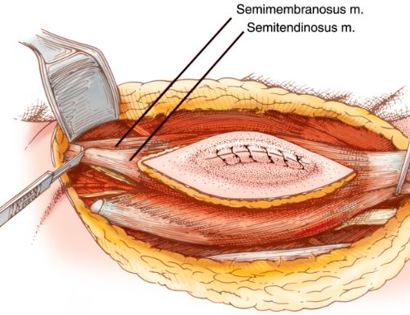
The entirety of the tumor is removed with margins to ensure that there isn't any tumor left in the area. The tumor is marked by the skin flap ellipse as seen in the image.
In cases that require vascular and muscular reconstruction, the sartorius or quadriceps muscles may be utilized.

We then close your incision with sutures and cover the surgical site with bandages. Multiple large drains may also be used to drain the surgical site and prevent a seroma (buildup of fluid).
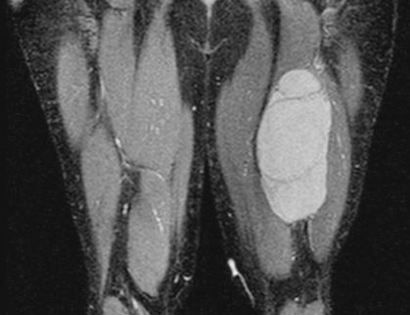
This is an MRI of the hamstrings tumor. The tumor is the brightened part on the right hand side of the thigh in the image seen.
Removal of tumor and reconstruction. Once the tumor is properly removed, the defect (space where hamstring muscles were) may be filled depending on the size of the tumor and if vascular (veins and arteries) reconstruction was warranted.
After your surgery you will spend a few nights in the hospital and then will be recuperating at home. Various pain protocols and nerve blocks are used to minimize pain. Mostly all patients are very comfortable after the surgery. For the first few days you will ice the area and keep it elevated to reduce swelling. You will return to the office 2 weeks after surgery. Once cleared, you will subsequently start physical therapy. We usually prescribe specific physical therapy protocols 3 times a week for 12 weeks after surgery to gradually strengthen muscles. Strengthening with significant resistance after sufficient range of motion is achieved as determined by Dr. Wittig. There may be an ultimate weight limit imposed upon you depending on various factors.
You will be monitored periodically with MRI imaging over the course of 5 years to ensure there are no signs of recurrence. You will have follow up appointments every 4 months for the first 2 years, then every 6 months for the next 2 years, and then once a year. Since the integrity of the limb has been restored to full or almost full, recovery is anticipated provided the patient adheres to strict physical therapy.

Dr. James Wittig narrates a video illustrating the surgical technique for resection of a tumor of the posterior thigh (Hamstrings). | WATCH VIDEO