What is Limb-Sparing Surgery of the Upper Femur/Hip?
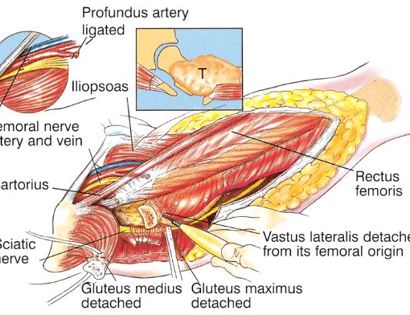
The hip consists of your femur and pelvis. The pelvis is composed of three parts; the ischium, ilium, and pubis. The socket (hip joint) is called the acetabulum which forms the “cup.” The proximal (upper portion) femur and its diaphysis (middle portion) are common sites for primary bone sarcomas and metastatic tumors. Some of these tumors include osteosarcomas, chondrosarcomas, and Ewing’s sarcomas. Limb-sparing surgery can be performed for approximately 95% of tumors arising from the upper femur. In some instances, the extremity cannot be saved and an amputation is performed.
Contraindications for saving the limb may include neurovascular invasion, infection, pathological fracture, invasion of the pelvis, extensive disease, contamination from a poorly performed biopsy, recurrent disease.