What is Intralesional Curettage and Bone Grafting?
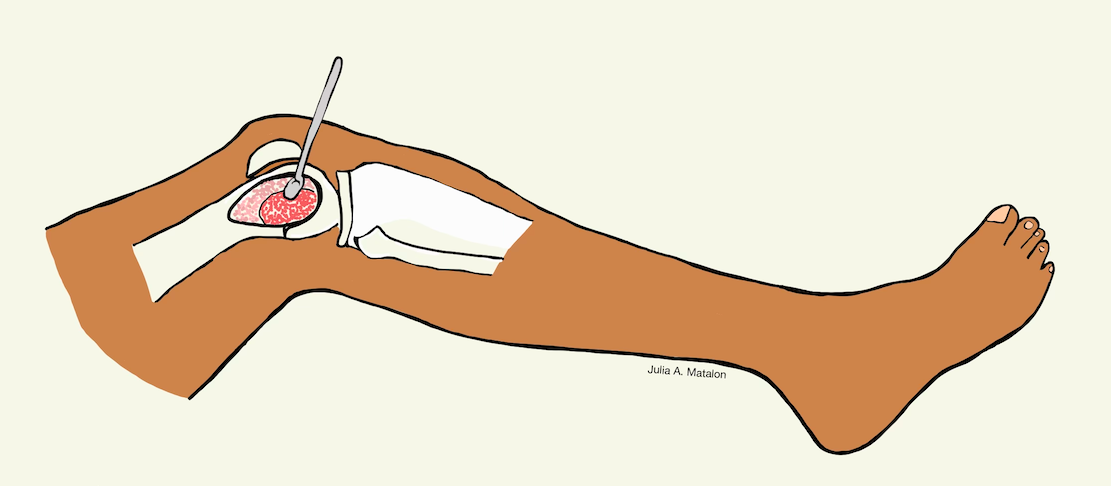
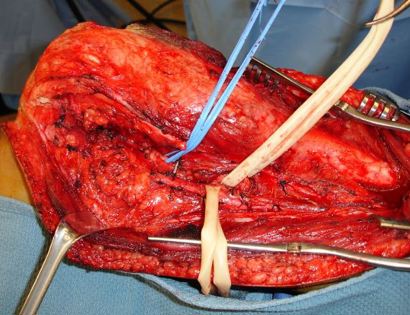
Intralesional Curettage means to scoop the tumor out using a spoon-like tool called a curette. This is a surgery that aims to remove the mass and restore the bone so that the patient can get back to normal function. The tumor is identified within the bone and scooped, or curetted, out.
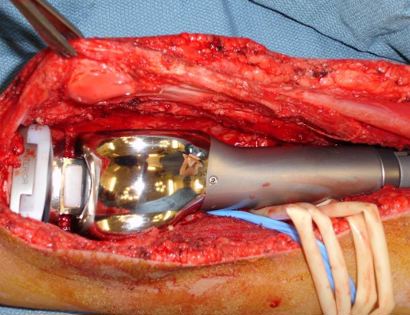
Bone Grafting and Fixation means that the empty bone cavity is filled with bone graft or bone cement. Bone can be donated (allograft) or taken from the patient themselves (autograft). Fixation devices, such as a plate and screws, may be used in specific situations to prevent postoperative fracture. This example of an X-ray shows the bone graft filled in nicely. It looks particulate. In this case, the patient was placed in a cast to protect from fracture and allow the graft to heal.