Osteoblastoma
A rare, noncancerous but aggressive tumor that produces bone. If left unchecked, it will continue to grow and destroy the bone. Surgical treatment is preferred. There is a high risk of recurring, or coming back, after removal.
A rare, noncancerous but aggressive tumor that produces bone. If left unchecked, it will continue to grow and destroy the bone. Surgical treatment is preferred. There is a high risk of recurring, or coming back, after removal.


A rare, benign and aggressive tumor that produces bone. Osteoblastomas are rare tumors and constitute about 1% of excised primary bone tumors.




Osteoblastomas are noncancerous but aggressive tumors that, if left unchecked, will grow and destroy your normal bone and invade the surrounding tissues. Clinically, local pain and swelling may be the first signs of an osteoblastoma. They have a high risk of recurring (coming back after removal) especially in the spine.
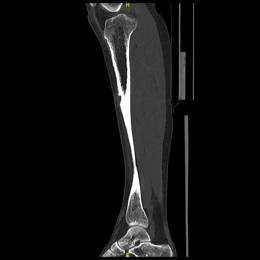
Radiographic imaging is used to help form a diagnosis. These include X-Ray, MRI, CT and Bone Scans.
An example of an CT is shown.

In the long bones, surgery usually consists of an intralesional curettage with burr drilling combined with bone graft and/or bone cement and possible fixation with some form of plates and screws or intramedullary rods. Since these have a risk of recurring other adjuvants such as liquid nitrogen or argon beam ablation are also often utilized to kill microscopic cells and minimize the risk of the tumor coming back. In the spine, a wide en-bloc resection is usually performed whenever possible. En-bloc means to remove in one piece with surrounding normal bone. Cryosurgery and argon beam are usually not performed given the proximity to spinal canal or important nerves. Spinal stabilization may be required if the removal destabilizes the spine.
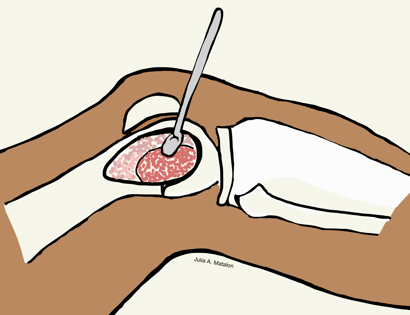
Intralesional Curettage means to scoop the tumor out using a spoon-like tool called a curette. This is a surgery that aims to remove the mass and restore the bone so that the patient can get back to normal function. The ABC is identified within the bone and scooped, or curetted, out. The cavity is then shaved down with a Midas Rex Drill, which is similar to a dental drill. This drill removes more tumor cells.
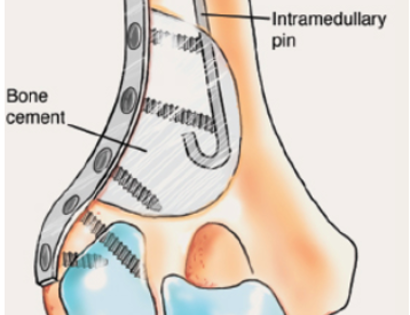
The empty bone cavity is usually filled with bone graft or bone cement. Bone can be donated (allograft) or taken from the patient themselves (autograft). Fixation devices, such as a plate and screws, may be used in specific situations to prevent postoperative fracture. This example of an X-ray shows the bone graft filled in nicely. It looks particulate. In this case, the patient was placed in a cast to protect from fracture and allow the graft to heal.

I've seen many doctors and I can confidently attest Dr. Wittig is the preeminent orthopaedic specialist. He is genuinely kind and caring, as he demonstrated by completely addressing my concerns and compassionately relating to what I was dealing with. He clearly outlined the plan of attack, and recommended the two additional doctors who would become part of my 'team'. Dr. Wittig was so effective in allaying our fears and bringing us optimism. My surgery was significant, but I was up and walking the next day and back at the gym 5 weeks later. This is further testament to Dr. Wittig's skill. He saved my leg and my life, and I feel so very blessed to say he is my doctor. I have already recommended him to others, and I will continue to do so. I would trust him with my closest family and lifelong friends. BEST DOCTOR EVER.
S.G.

Myself and my amazing team are dedicated to saving your life and your limb. Losing a limb because of a tumor can be a terrifying experience. But, it does not have to be the only option. I’ve spent 20+ years as a Board-Certified Orthopedic Surgeon and Orthopedic Oncologist.
I’ve devoted my career to helping children and adults afflicted with bone and soft tissue masses by performing complex limb saving surgeries. Most patients can have their limb saved, which may require innovative techniques.
Patients afflicted with musculoskeletal tumors have complex conditions that are best taken care of at large hospitals. I am the Chairman of Orthopedics and Chief of Orthopedic Oncology at Morristown Medical Center. My philosophy is a multidisciplinary team approach, working together to tailor treatment to individual patients. Education and research are essential to my practice, providing the best setting for extraordinary patient care. Because of this, we have some of the top results in the country.
